Article Text

Statistics from Altmetric.com
Introduction
The COVID-19 pandemic is a child rights crisis challenging long-term survival and development of children and youth worldwide. The pandemic and indirect consequences of associated public health measures are compounding pre-existing stressors to survival that marginalised families confront every day, with detrimental and disproportionate consequences. Service shutdowns, reduced healthcare access, disrupted early childhood education and schooling and long-term economic decline will be more harmful to children than the virus itself. The International Society for Social Pediatrics and Child Health (ISSOP) is a global organisation of health professionals that aims to improve the health and well-being of children and young people with a focus on the child, in illness and in health, within the context of their society, environment, school and family. This ISSOP Position Statement outlines the impact of COVID-19 to child and youth health inequities and calls for action by governments, health professionals, researchers and advocacy organisations.
Statement of the problem
The COVID-19 pandemic will amplify inequity unless we act to ensure it does not
Improvements in the health and well-being of children and youth over the past 20 years, in part driven by the Millennium and Sustainable Development Goals, are at risk of being reversed, with widening inequities within and between countries.1 In low-income and middle-income countries (LMICs), the pandemic places an additional burden on fragile financial and health systems with pre-existing resource constraints.2 3
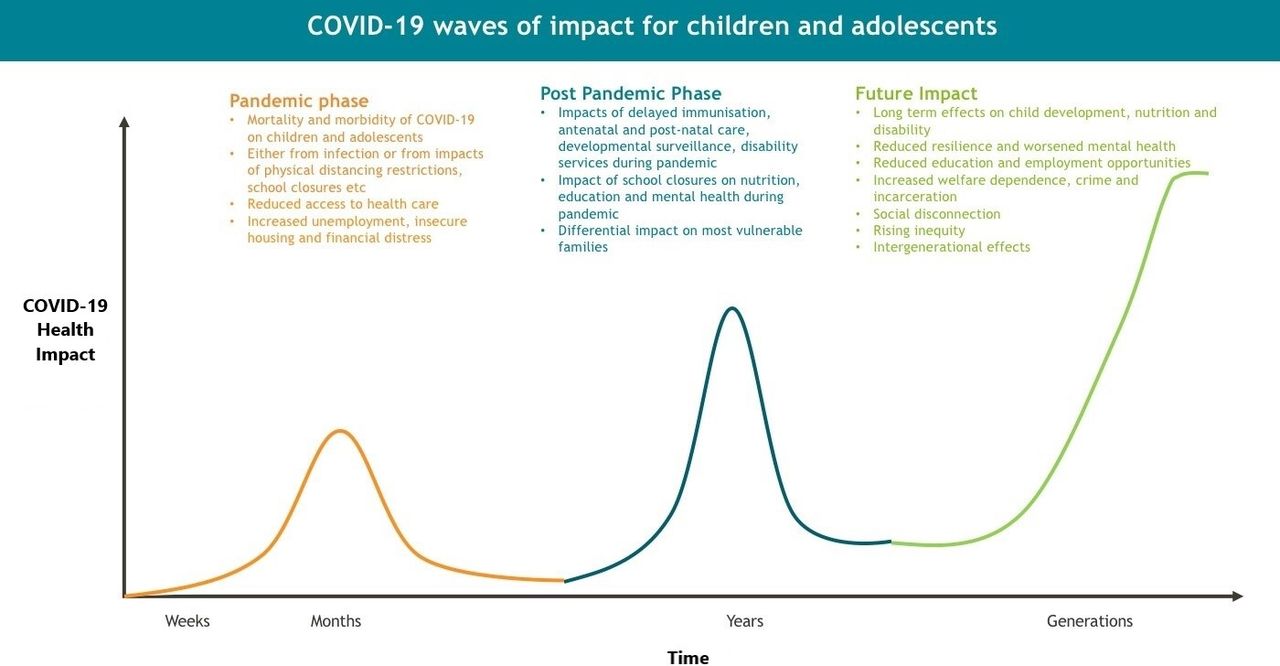
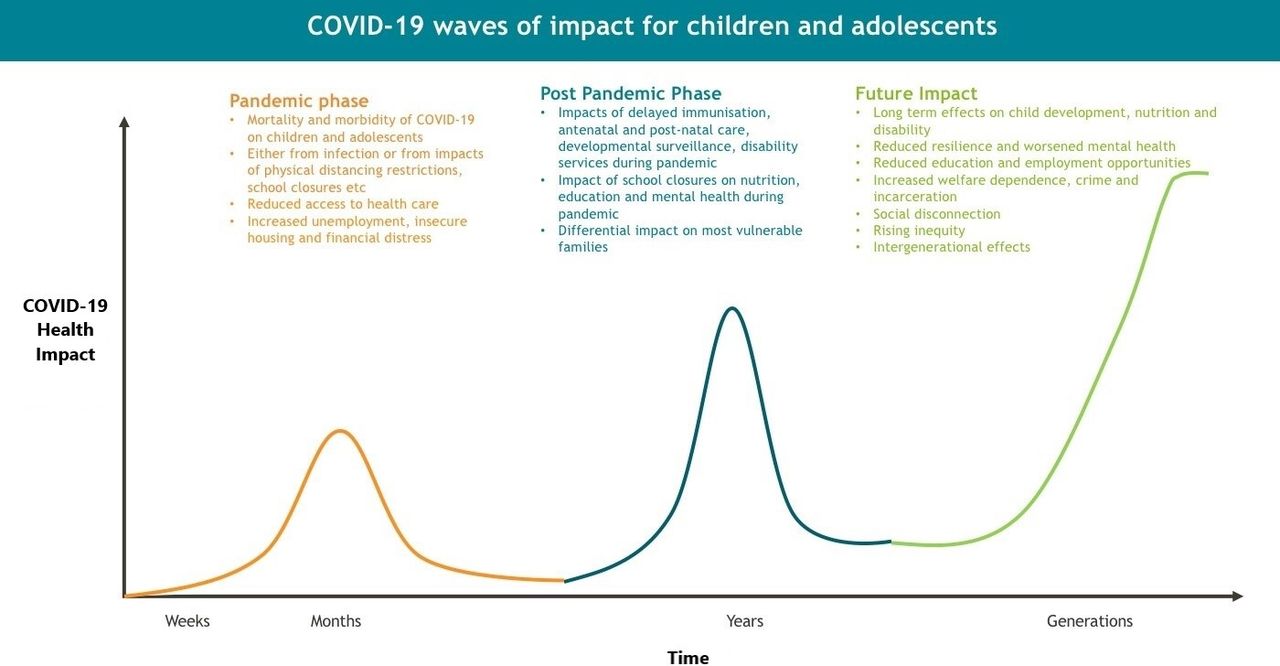
In the short term, disrupted access to health, education and social services worsen health outcomes in disadvantaged children and youth.3 However, longer term impacts on health, well-being, literacy, income, professional opportunity, housing and intergenerational effects are potentially devastating4 (figure 1).
{kind=link}
COVID-19 waves of impact for children and adolescents.
A child rights-based approach to defining the impact of the COVID-19 pandemic on children
Rights articulated in the United Nations Convention on the Rights of the Child, adopted by all countries except the USA, have been difficult to uphold during the pandemic.
Right to health and access to healthcare (Article 24)
Multisystem disruptions due to lockdowns, travel restrictions and fear decrease access to antenatal care, early childhood development programmes, and basic health and human services.4
Hospital births have declined by 21% in India and some African countries. Postpartum separation has decreased breastfeeding rates in many parts of the world.2
Visits to healthcare facilities have declined and immunisation programmes suspended globally, with a 69% reduction in measles, mumps and rubella vaccination in India.1 Breakthrough wild and vaccine-derived polio cases emerging prior to the pandemic have escalated this year.2
Disruption of supply chains and cost has restricted procurement of soap, hand sanitiser, diagnostic testing, medicines, face masks and other personal protective equipment (PPE) while countries have seen endorsement of unproven herbal or chemical remedies.2
Right to education (Article 28)
Disruption to education and school support has potential for lifetime impacts on human capability in all settings. School closures sever precarious connections to education and school-based social supports, reducing education and employment opportunities and potentially leading to juvenile justice involvement and unemployment.4 School closures have greater impact in children with disabilities and learning difficulties and in LMIC with reduced access to online learning.3
Right to live free of exploitation: child labour, drug abuse, sexual exploitation, abduction, recruitment, trafficking or any activity that could harm welfare or development (Articles 32/34/35/36). Protection from violence, abuse or neglect (Article 19)
Loss of access to school, constructive recreational opportunities and closure of children’s facilities have reduced children’s protection and enhanced risk of child abuse, unregulated labour and combatant recruitment among teenage boys in LMIC.1 5
Financial distress, reduced extrafamilial observation and overwhelmed child protective services globally have resulted in increased domestic violence and sexual and gender-based violence, with girls at higher risk of sexual exploitation and abuse, increased child marriage and less likely to return to school, further widening gender gaps.1 5
The best interests of the child a primary consideration (Article 3). Right to optimal survival and development (Article 6). Right to adequate standard of living that supports mental and physical needs (Article 27).
Differential impacts on children and youth living in poverty are expected due to greater dependence on the informal economy, fewer financial reserves, reduced access to technological solutions for healthcare and education and high levels of psychological distress.1
Overcrowded communities in LMIC with no piped water are unable to adhere to physical distancing or handwashing regulations.2
Hunger has been exacerbated by reduced caregiver income and closure of school feeding programmes, soup kitchens and government food distribution.1
In HIC, children in low-income and ethnic minority households are at increased risk of adult deaths, leaving households without one or more caregivers.3
Are there opportunities to use the pandemic to reduce inequities, harness the positive and build a sustainable future?
Reducing child poverty, addressing determinants of health and strengthening health systems to ensure universal health coverage will advance the rights of children and youth and improve global health and well-being.1 3 Innovative health and welfare solutions that have arisen during the pandemic could help accelerate this ideal.
In Kerala, India, networks of women’s groups have created PPE, established community kitchens and provided educational, leisure and counselling interventions for children.
In Senegal, cheap diagnostic tests have been developed; in Ghana and Kenya, local supplies of masks have been created.
In Somalia, student social workers have enhanced child safety in the context of workforce shortages.
In HIC settings, increased telehealth skills are creating more accessible healthcare delivery in remote, inaccessible areas. Many countries have expanded the reach of social safety net, homeless, financial and employment support packages.4 Measures to mitigate housing instability, the burden of rent and mortgage payments and evictions have been implemented.1
Of particular global importance, the pandemic has caused a reduction in carbon emissions and improved air quality. Also, the United Nations Network on Migration has recommended nations impose a moratorium on immigration detention.
Recommendations for action
ISSOP acknowledges the challenges during the pandemic but nonetheless urges governments, child health providers, researchers and advocacy organisations to respond urgently and definitively using a child rights-based response.
Governments
Direct resources to the care and protection of children and youth.4
Prevent food scarcity and hunger; support local food production.2 3
Support early childhood education.5
Ensure access to health, education and welfare services.1 3
Provide access to housing, water and sanitation.1
Control unregulated child labour, child abuse and early marriage. Invest in social infrastructure and workforce in education, health and social care for vulnerable children and youth.3
Combine emergency social protection responses with transitions into permanent programmes.1
Expand and protect employment.1 3
Establish financial support programmes, universal basic minimum wage or other strategies to support families.3
Ensure marginalised groups, including asylum seekers, have equitable access to services and benefits.1
Paediatricians and child health providers
Preserve and enhance routine maternal, child and youth health services, with equity as a specific objective.1 2
Affirm the dignity and rights of children and youth.3
Advocate for access to healthcare, protective services, housing, welfare and employment policies that support children and families.3
Enhance accessible and resilience-building mental health services for families.3 5
Develop telehealth and technologies that are sustainable and adapted to the specific environment.3
Maintain ‘eyes on the child’ and deliver essential services face to face where required.3
Researchers and advocacy groups
Advance child rights, social justice and health equity.1 5
Collaborate with key partners across the globe to discover and disseminate evidence to mitigate pandemic impacts on children and youth.3
Ensure that children and youth in LMIC benefit from research findings, immunisation and treatment options for COVID-19.
Mobilise international professional societies and work with civil society, especially children and youth, in all aspects of the pandemic.3
Conclusion
Deaths due to COVID-19 will be a small proportion of future global child deaths. Most deaths will result indirectly from poor access to nutrition, housing, water and sanitation, vaccines and universal healthcare. This ISSOP declaration gives clear actions to ensure the pandemic does not worsen existing health inequities with lifelong and intergenerational consequences for children and youth. This pandemic must not impede the fragile progress made over decades in child and youth health and well-being but should act as catalyst for a more just and equitable world.
Ethics statements
Patient consent for publication
Footnotes
Twitter @Dr Lulu N. Oguda
Collaborators Karen Zwi, Jeffrey Goldhagen, Nicholas Spencer, Sharon Goldfeld, Susan Woolfenden, Benjamin Jones, Brendan Ross, Bernadine Ekpenyong, Angela Okolo, Christopher Yilgwan, Laurien Sibomana, Oladele Olatunya, Bosede Adebayo, Angela Osei-Bonsu, Rajeev Seth, Ilisapeci Vereti and Shanti Raman, on behalf of the International Society for Social Pediatrics and Child Health (ISSOP) COVID-19 Working Group.
Contributors RK undertook writing up and was responsible for the overall content. LO and OA assisted with writing up and contributed data on effects of the pandemic.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.