Article Text

Abstract
Objective To identify parents’ prioritised outcomes by combining qualitative findings from two trial feasibility studies of interventions for paediatric suspected severe infection.
Design Qualitative synthesis combining parent interview data from the Fluids in Shock (FiSh) and Fever feasibility studies. Parents had experience of their child being admitted to a UK emergency department or intensive care unit with a suspected infection.
Participants n=: 85 parents. FiSh study: n=41 parents, 37 mothers, 4 fathers, 7 were bereaved. Fever study: n=44 parents, 33 mothers, 11 fathers, 7 were bereaved.
Results In addition to survival, parents prioritised short-term outcomes including: organ and physiological functioning (eg, heart rate, breathing rate and temperature); their child looking and/or behaving more like their normal self; and length of time on treatments or mechanical support. Longer term prioritised outcomes included effects of illness on child health and development. We found that parents’ prioritisation of outcomes was influenced by their experience of their child’s illness, survival and the point at which they are asked about outcomes of importance in the course of their child’s illness.
Conclusions Findings provide insight into parent prioritised outcomes to inform the design of future trials investigating treatments for paediatric suspected or proven severe infection as well as core outcome set development work.
- paediatrics
- outcomes research
- severe infection
- clinical trials
- parents
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
The evaluation of interventions for the treatment of children with suspected or proven severe infection has been hampered by the underdevelopment of outcome measures.
The selection of clinical trial outcome measures is predominantly led by clinicians and researchers rather than by patients and their families.
Research is needed to ensure the selection of outcomes in trials investigating treatments for paediatric severe infection reflects the priorities of families.
What this study adds?
Our synthesis showed that in addition to survival, parents prioritised short-term outcomes including: organ and physiological functioning (eg, heart rate, breathing rate and temperature); their child looking and/or behaving more like their normal self; and length of time on treatments or mechanical support.
Longer term prioritised outcomes included effects of illness on child health and development.
Parents’ prioritisation of outcomes was influenced by their experience of their child’s illness, survival and the point at which they are asked about outcomes of importance in the course of their child’s illness.
Introduction
Severe infections remain a major cause of mortality and morbidity in paediatric clinical care.1 International research prioritisation exercises2–4 highlight the need for research to explore which interventions may improve patient outcomes for paediatric severe infection. However, little knowledge exists about which outcomes are most important to parents of children treated for severe infection requiring fluid resuscitation and/or intensive care admission.5 6
Despite recognition that patients and the public have a legitimate and requisite role in the design and conduct of health research, the extent to which this occurs is less clear.7 8 Two systematic reviews7 9 of outcome measures in clinical trials suggest that they are predominantly selected by clinicians and researchers. Sinha et al 9 observed that only 3 out of 13 groups who had published on the selection of outcomes for paediatric clinical trials had consulted parents; none involved children.
To inform the design of two trials involving children with suspected severe infection, we used qualitative research to explore parents’ views on trial acceptability and important treatment outcomes. This paper presents combined qualitative findings from the Fluids in Shock (FiSh) and Fever studies (see table 1) on parents’ prioritised outcomes.
Overview of the Fluids in Shock (FiSh) and Fever feasibility study designs
Methods
FiSh and Fever studies took place between 2015 and 2018. Both began with a qualitative feasibility study, led by the same qualitative research team (phase 1). This involved semistructured interviews with parents (including bereaved parents) of children who had attended UK emergency departments (EDs) or were admitted to a paediatric intensive care unit (PICU) with severe infection in the previous 3 years. Phase 1 informed the design of pilot trials (phase 2; 9-month recruitment period in FiSh and 4 months in Fever), which had an integrated interview element involving parents of randomised patients.
We used previous research10–12 to develop interview topic guides to explore parents’ views on trial design and conduct,13 including outcomes for the proposed definitive trials (see online supplementary table S1). To inform discussions with parents (phase 1), we conducted a literature review to develop a list of outcome measures previously reported in paediatric severe infection research.
Supplemental material
Recruitment and interview conduct
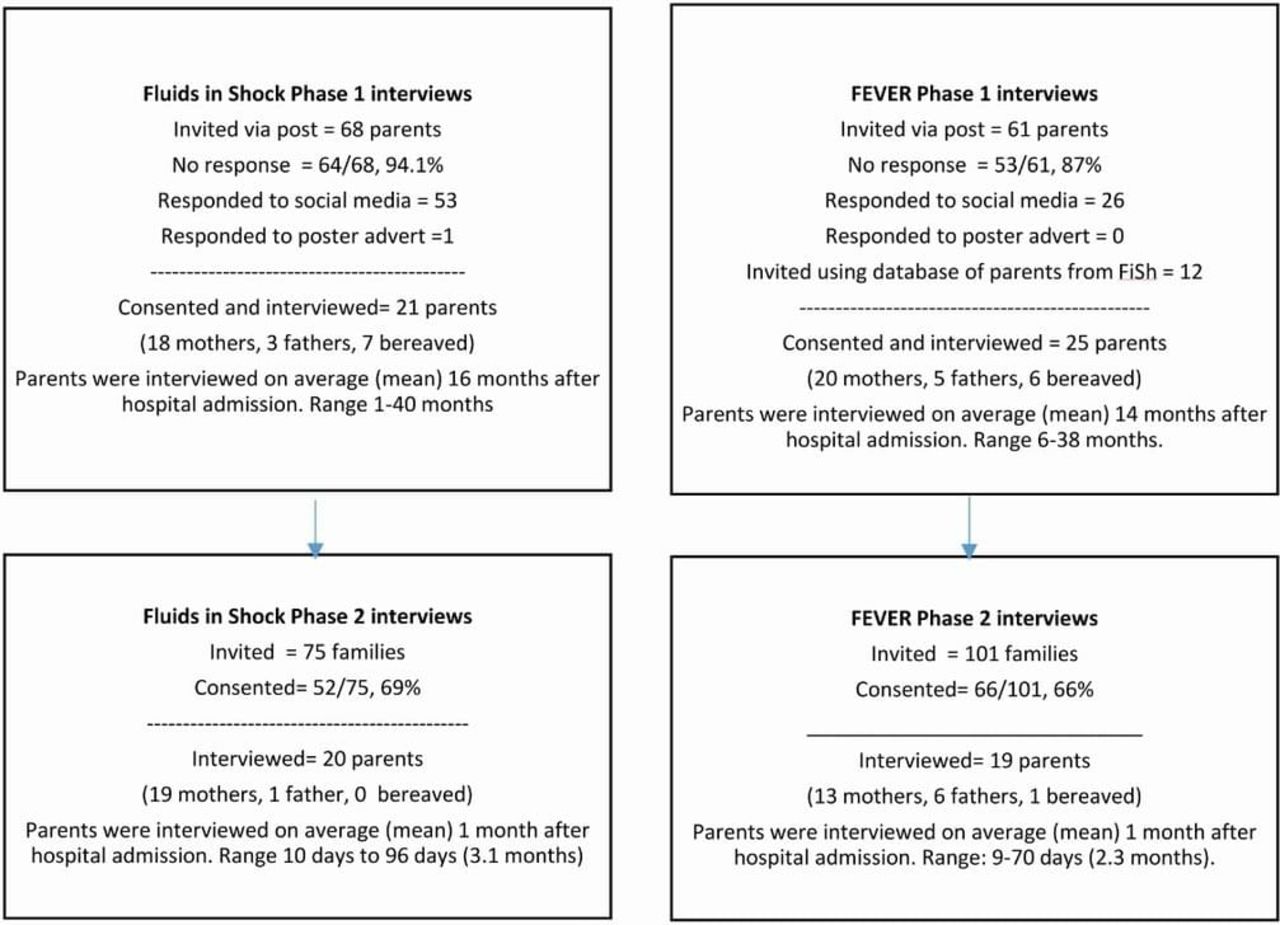
Based on previous studies14 15 we anticipated needing 15–25 parents for each qualitative study phase (see figure 1). In phase 1 studies, parents were recruited through postal contact, advertising in EDs and PICUs and online including social media.13 A database of FiSh potential participants who consented to contact about future studies but had not taken part in an interview in FiSh were approached to participate in Fever. In phase 2 studies, clinicians provided parents with information and sought consent to contact for interviews as part of the FiSh and Fever pilot trial consent discussion.

{kind=link}
Participant recruitment and sample characteristics by study and phase.
In phase 1, expressions of interest to participate were responded to sequentially. Selection of parents for interview aimed to ensure variance of recruitment method (eg, social media, postal/database invitation and poster advert). The list of potential outcomes was emailed to parents to read prior to interview. Verbal consent was audio recorded. In phase 2, CO, ED or KW contacted parents within 1 month of consent or hospital discharge. Selection of parents for interview aimed to include all pilot sites and range of parent experience (eg, consented and declined the trial and trial arm allocation). Consent for audio recording was confirmed. In both phases, parents were asked to reflect on their personal experiences to identify important outcomes for future trials (see online supplementary table S1). Screening and interviews stopped on reaching data saturation (see online S2 box 2 for a glossary of terms).16 17
Supplemental material
A professional transcription company (Voicescript Ltd, Bristol, UK) transcribed verbatim digital audio recordings. Transcripts were anonymised and checked for accuracy.
Data analysis and synthesis
Psychologists CO (PhD, female research associate FiSh) and ED (PhD, female research associate Fever) led the analysis with assistance and oversight from KW (sociologist). Analysis for each study was broadly interpretive, inductive and iterative14 18 as informed by the constant comparative approach.19–22 Outcomes were identified through direct questioning as well as referred to indirectly by parents during wider interview discussion.
NVivo V.10 software (QSR International Pty Ltd, Melbourne, Australia) was used to assist in the organisation and coding of data. CO, ED and KW met regularly to discuss interpretation and develop the coding framework. To present a prioritised list of outcomes for each study phase, we listed outcomes in order of how commonly they were discussed by parents. Outcomes discussed through direct questioning were placed higher in the list than outcomes identified in general interview discussions. Lists for FiSh and Fever phases 1 and 2 were then merged.
Results
Sample
We interviewed 85 parents (82 via telephone, 3 face to face), including 41 (37 mothers, 4 fathers) from the FiSh study and 44 (33 mothers, 11 fathers) from the Fever study (figure 1). Only the researchers and participants were present. Fourteen parents were bereaved (13 from phase 1 studies and 1 from phase 2). We reached data saturation point16 17 at 21 (FiSh) and 25 (Fever) interviews in phase 1 and 20 (FiSh) and 19 (Fever) interviews in phase 2. Due to the different recruitment designs, parents in phase 1 studies were interviewed at a later time point after their child’s hospital admission than parents in phase 2 studies (see figure 1). Interviews took between 30 min and 55 min.
Outcomes of importance to parents of children with severe infection
Many outcomes discussed by parents during interviews mapped closely to outcomes identified in the literature review. Parents often prioritised multiple outcomes (eg, in FiSh phase 1, an average of six outcomes, and seven outcomes in phase 2).
Online table 2 (S3) shows outcomes identified in the analysis of FiSh and Fever interview transcripts. Outcomes are ranked in order of importance, defined as how many parents mentioned a particular outcome when asked directly which indicators were most important to them.
Supplemental material
Parents did not always view treatment outcomes for severe infection as a set of independent constructs. Many described important indicators of improvement as lying on a continuum, or ‘gradient of seriousness’ (P6, mother, non-bereaved, FiSh phase 1). Initially looking for ‘the worst [outcome] and then… you sort of progressively aim towards the sort of next hurdle to get over’ (P10, mother, non-bereaved, FiSh phase 1).
The most commonly prioritised outcomes are presented with illustrative quotations in table 2.
Illustrative quotes for the top five prioritised outcomes
Improvement in organ and physiological function
Thirty-eight parents (38/85, 45%) described the importance of noticeable improvements in their child’s organ functioning and core physiological parameters as short-term treatment outcomes. These included heart rate, temperature, dehydration, blood pressure and respiratory rate.
Looking and behaving like normal self
The concept of a general, overall feeling of return to health or normality was referred to by 33/85 (40%) parents. Parents described this as an improvement in their child’s appearance and temperament. For those with sepsis, this included a reduction in the magnitude of swelling and skin discolouration. Improvements in child temperament included references to behaviour and mood, including increased alertness and decreased irritability. These outcomes were linked to improvement in other core functions of life, including ‘feeding’ (P49, mother, non-bereaved, Fever phase 2), ‘talking’ (P19, mother, non-bereaved, FiSh phase 2) and ‘walking’ (P20, mother, non-bereaved, FiSh phase 1). Together, improvement in these symptoms was taken as an important indicator to parents that their child was recovering and on the road to ‘looking more like herself’ (P13, mother, non-bereaved, FiSh phase 1).
Long-term health and development
Parents of recovered children (22/71, 31%) described how their child’s health status following hospital discharge was an important indicator of treatment efficacy. Prioritised outcomes included global development and functioning and quality of life. Health status was almost always spoken of in terms of the overall impact it had on their children’s lives and future experiences (eg, the impact of limb amputation). These outcomes featured more strongly for parents in the phase 1 FiSh and Fever studies. Only one phase 2 study participant indirectly referred to long-term effects. This suggests that priorities may evolve with the passage of time after a severe illness.
Reduced need/time spent on treatments and mechanical support
A reduction in the number of machines supporting their child, including duration of or need for mechanical support was described (21/85 parents, 25%) as an important short term outcome. This included time on machines (eg, ventilator and extracorporeal membrane oxygenation ECMO) and medications (eg, morphine).
Length of hospital stay
Seventeen parents (17/85, 20%) discussed length of stay in hospital as an important outcome to measure. Six parents (three in FiSh, three in Fever) prioritised length of intensive care stay.
Survival
Survival was often prioritised by bereaved parents over all other outcomes yet was rarely described by parents of recovered children in FiSh and phase 1 of Fever. We amended the Fever phase 2 topic guide to explore all parents’ views on survival as an outcome after they had prioritised outcomes. Following prompting, an additional seven parents described survival as the most important outcome measure for the proposed RCT and future-related trials. Reasons why they had not initially mentioned survival included death either not being something they had wished to consider or had not considered as their child had survived (see table 3). Others had not perceived their child’s condition to be life threatening (eg, bronchiolitis).
Reasons why survival had not been initially prioritised by parents
Discussion
Our findings provide new insight into parent-prioritised outcomes for paediatric emergency medicine or intensive care trials investigating treatments for severe infection. In addition to survival, parents-prioritised short-term outcomes include: organ and physiological functioning; their child looking and/or behaving more like their normal self; and length of time on treatments or mechanical support. Longer term prioritised outcomes included physical and developmental effects of illness on the child.
Consistent with outcomes used in previous trials in this condition,23–25 parents prioritised improvements in their child’s organ and physiological functioning as an indicator of treatment efficacy and recovery. Specifically, parents favoured the alleviation of core infection-associated symptomatology, such as heart rate, temperature and respiratory rate, increase in blood pressure and hydration. Parents frequently referred to their observation of monitoring displays and treatments their child received. Linked to these outcomes was time to liberation from therapeutic treatments and machines, particularly mechanical ventilation. These outcomes were important, as a reduction in their number and required usage (eg, time) was viewed as an indication that their child was getting better.
The ideal outcome measure in septic shock has been described as ‘patient centred, easily measured, and clinically important’,6 while longer term outcomes are often not prioritised due to the practical and financial costs of collecting such data. If trial findings are to be impactful in ensuring patient centred healthcare26 27 and influencing policy and practice, then they must be relevant and important to patients and families.11 28 Long-term effects of severe infection, such as physical and developmental consequences, and the short-term outcome of ‘looking and behaving more like normal self’ are not easily measured and would rely on parent reports. Nevertheless, this should not preclude their consideration or inclusion. Indeed, ‘looking and behaving more like normal self’ was the second most commonly prioritised outcome across both studies. To our knowledge, there is no validated tool for this outcome. Scales such as the Pediatric Overall Performance Category,15 Children’s Critical illness Impact Scale29 and Functional Status Score30 could help measure some of the functional morbidity and behavioural outcomes described. However, they do not capture parents’ perspectives on outcomes observed during their child’s PICU stay. Further work is needed to define and develop this parent prioritised outcome measure.
Survival was prioritised by bereaved parents over all other outcomes. However, in many interviews with non-bereaved parents, survival was only prioritised after specific prompting. Our findings showed that parents had either not perceived their child’s life to be at risk, had high expectations of healthcare treatments or had not wished to consider the death of their child as a possible outcome. This suggests that some parents either did not fully comprehend the severity of their child’s illness,31 or they had developed adaptive coping behaviours to seek agency over the stressful situation by not considering death as a possibility.32 33 However, as mortality rates related to severe infection are declining in most affluent countries, morbidity-related outcomes may be the most appropriate focus for future trials investigating severe childhood infections.6 34
Interestingly, the point at which parents were asked about outcomes in the course of their child’s illness appeared to influence prioritisation. This suggests the need for the development of a core outcome set to include patients/family members with a range of relevant experiences for that condition and to include participants at different time points in the course of their, or their child’s, illness. This list of parent-centred outcomes can be used in future core outcomes set consensus work (see online S3 table 2) involving all key stakeholders (eg, clinicians, parents and children). Consensus methodology could also be used to identify the optimal duration of follow-up in these studies, including which outcomes to measure at short-term and longer term time points.
Strengths, limitations and future implications
Our findings contribute to an important and under-researched area and demonstrate the value of using qualitative methods to explore parents’ perspectives on outcome measures. Synthesis of study findings was strengthened by harmonised study designs, topics guides and processes, which were developed and conducted by the same expert team. Recruitment in each phase was conducted until data saturation was reached,16 17 and both bereaved and non-bereaved parents with varying experience of their child being treated for severe infection were included, providing new insight into how views on outcomes may change with illness severity and trajectory. As the majority of FiSh and Fever participants were infants (eg, in Fever 64% were <1 year old), our insight into important outcomes for paediatric septic shock is limited to the views of parents. Future research is required to explore children’s views on important outcomes in emergency and critical care trials.
The list of outcomes compiled from the FiSh literature review was presented to parents in the phase 1 studies. Use of a list may have influenced their views on outcomes. Nevertheless, common themes were identified within and across phases of FiSh and Fever studies and similarities between suggested outcomes and the predefined set were evident. Finally, more interviews were conducted with phase 1 parents (n=46) compared with phase 2 parents (n=39), which may have biased the order of combined outcomes towards phase 1 parents’ priorities.
Conclusions
Our findings provide insight into short-term and long-term outcomes prioritised by parents to inform the design of future trials investigating treatments for paediatric suspected infection as well as core outcome set development work. In addition to survival, parents prioritised organ and physiological functioning their child looking and/or behaving more like their normal self; length of time on treatments or mechanical support, and long term and effects on child development.
Acknowledgments
The authors would like to thank all the parents who shared their experiences with us; their contribution to the research is invaluable. The authors are grateful to all the staff at participating UK hospitals and charities/support groups for their help with recruitment. The authors would also like to thank the Paediatric Emergency Research in the UK and Ireland (PERUKI) and Paediatric Intensive Care Society (PICS) for their support and contribution to the development of this research.
References
Footnotes
Contributors DI, MJP, KW, PM, RC, IK and KMR conceived and designed the research. All authors contributed to the study design of recruitment materials and topic guides. CBO, ED and KW conducted the interviews. CBO, ED and KW analysed the data. CBO, KW, ED, DI and MP wrote the paper. MDL, PM, LT, RA, and KT critically revised the manuscript. All authors reviewed and approved the final manuscript.
Funding This study was funded by the National Institute for Health Research (NIHR) Health Technology Assessment programme (Fluids in Shock (FiSh): 13/04/105, Fever: 15/44/01) and supported by the NIHR Great Ormond Street Hospital Biomedical Research Centre.
Disclaimer The views expressed are those of the authors and not necessarily those of the National Health Service, the NIHR or the Department of Health and Social Care. The funders had no role in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Competing interests None declared.
Ethics approval The FiSh feasibility study (phase 1) was approved by the North West – Liverpool Central Research Ethics Committee (15/NW/0913). The FiSh external pilot study (phase 2) received full ethical approval from the Health Research Authority (HRA) and was approved by London Stanmore NHS Research Ethics Committee (16/LO/0854). The Fever qualitative study (phase 1) was approved by North West – Liverpool East Research Ethics Committee (16/NW/0826). The Fever pilot trial received full ethical approval from the Health Research Authority and was approved by Hampstead NHS Research Ethics Committee (Reference number: 17/LO/1139).
Provenance and peer review Not commissioned; externally peer reviewed.
Collaborators Conducted on behalf of PERUKI and PICS.
Patient consent for publication Not required.
Patient and public involvement Patient partners AC, NJ and JW were involved in study design, oversight, review and interpretation of FiSh (AC and NJ) and Fever (JW) findings. All reviewed and approved the final manuscript.